Dentist – Gregory Cole, D.D.S.")
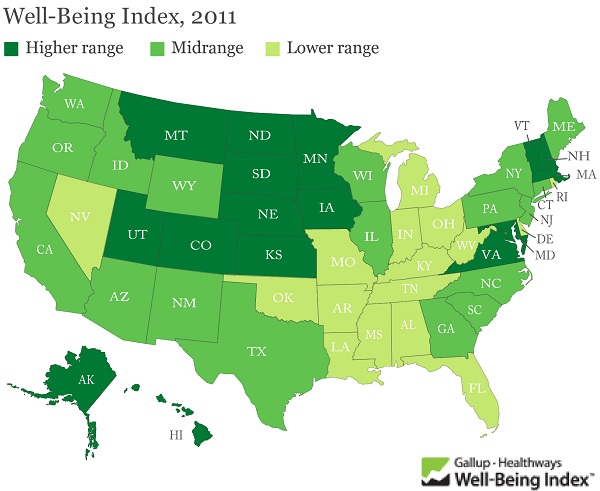
Poll Watch: Obesity and Chronic Diseases Stable Across the United States in 2011
Posted on
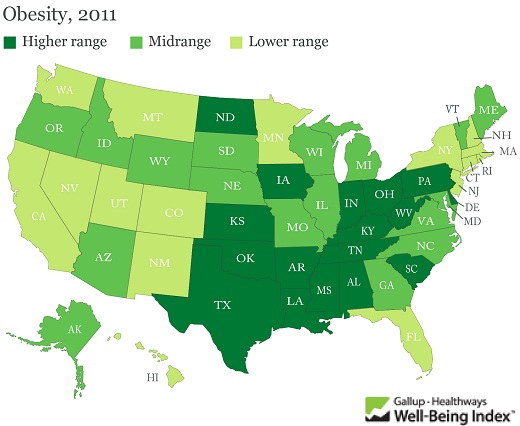
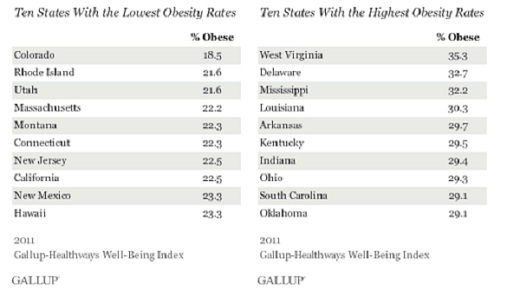
Colorado had the lowest adult obesity rate in the nation in 2011, as it did last year, and is the only state where fewer than 20% of adults are obese. West Virginia holds onto the negative distinction of being the state with the highest obesity rate; 35.3% of residents living there are obese, the highest for any state that Gallup and Healthways have found since 2008.
The national obesity rate declined slightly to 26.1% in 2011, from 26.6% in 2010. Across states, obesity rates remained statistically unchanged from 2010 to 2011 in all but two — New Jersey and Kentucky — where they declined. This marks a positive change from the recent past. Obesity had inched up in 2009 and 2010 compared with 2008 nationwide and in some states.
These data, collected as part of the Gallup-Healthways Well-Being Index, are based on respondents’ self-reports of their height and weight, which are used to calculate Body Mass Index (BMI) scores. Americans who have a BMI of 30 or higher are classified as obese.
The obesity rate continues high, but at least it did not increase this past year. Is the word getting out about the problem?
Here is a chart about the best and worst states:
It is interesting that the states in the South and the Midwest lag the other states and have higher rates of obesity and chronic diseases. They also have the higher rates of smoking.
There needs to be more awareness and education about the needs to eat right, exercise regularly and not smoke – for a more healthy and productive life.